Featured
Clinical Kit 103 - 'High' Ankle Injuries
This edition of Clinical Kit focuses on the less common but generally more troublesome 'high' ankle sprain - that involving the syndesmosis. New research looks at the correlation between MRI and palpation and finds that with a good knowledge of anatomy, your palpation skills are extremely diagnostic. Something that I am always banging the drum about. Oh - if you were wondering, you are welcome to attend one of our Living Anatomy Wet Labs to assist you in upskilling :) 
Assessment of the Injured Ankle in the Athlete
Then by way of an introduction into the specifics of why high ankle sprains require a high index of suspicion during clinical assessment seeSpecific article examining the ins and outs of a 'high' ankle assessment
Now for the main feature article.
Stable Versus Unstable Grade II High Ankle Sprains: A Prospective Study Predicting the Need for Surgical Stabilization and Time to Return to Sports.
Calder JD, Bamford R, Petrie A, McCollum GA
Abstract available here: http://www.ncbi.nlm.nih.gov/pubmed/26725452
Using the West Point Classification system of ankle injuries, the authors explain how they are interested in developing the grade 2 classification. Grade 1 is minor and conservative treatment is successful, grade 3 is a complete dislocation and requires surgical intervention. Their interest is in deciding what indicators could determine if a grade 2 should be managed conservatively (like a grade 1) and which ones operatively (ala grade 3).
West Point Classification System
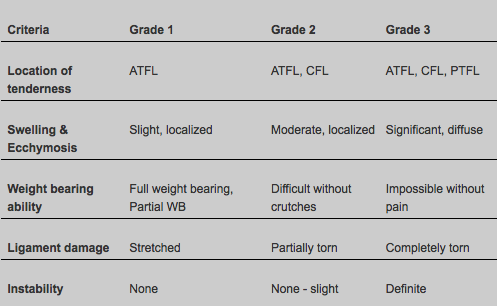
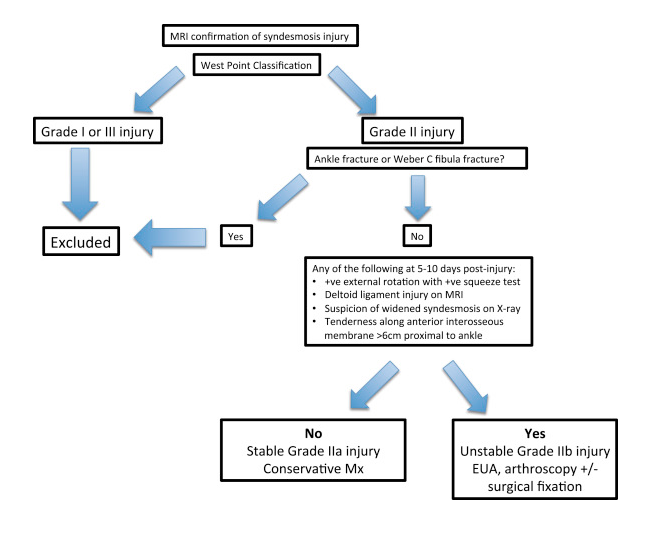
So they looked at criteria that could implicate the placement of grade 2 injuries into one of two classifications with a focus on intervention - conservative or surgery.
My Clarification
In this paper there is one confusing aspect that relates to the usage of the acronym ATFL. Usually the ATFL relates to the most commonly injured ligament in the lateral complex, the anterior talofibular ligament. In searching anatomical texts and sports medicine books, the ligament commonly relating to a syndesmosis injury, is the anterior inferior tibiofibular ligament (AiTFL), not the more general term anterior tibofibular ligament.
Furthermore in the Discussion section of this paper, the authors talk about the significance of the ATFL as a clinical predictor of recovery. When there is pain on palpation of the ATFL, this correlates to a lesser syndesmosis injury and quicker return to play (so clinically it is important). Their explanation being, "We presume that the mechanism of injury is different for these patients. When there is injury to the ATFL, it is primarily supination-inversion (the classical lateral ligament sprain)... Conversely, patients without an ATFL injury probably have a true syndesmotic disruption from the dorsiflexion external rotation mechanism". Remember supination is a triplaner term referring to plantarflexion, inversion and adduction). So when reading the following results you will need to consider what ATFL is referring to. I can't believe this anatomical error has been missed, so much so that I think I am wrong, yet at the same time it does seem wrong. If someone can enlighten me I would be very appreciative.
Grade IIa Management
Patients with a clinically stable syndesmosis (grade IIa) were treated nonoperatively and underwent placement of an Aircast XP Walker boot (DJO Global, San Diego, CA) while not bearing weight for 10 days, after which they were allowed to bear weight as long as pain free. The medical team was advised to leave the boot on for a minimum of 3 weeks and then to mobilize the ankle free of the boot as long as the ankle was pain free. Taping of the ankle syndesmosis was encouraged for a minimum of a further 6 weeks during the rehabilitation phase.
Grade IIb Post Surgery Management
Following surgical debridement and stabilization, the patients were mobilized in a boot for 4 weeks while non–weight bearing for 1 week, partially weight bearing for 1 week, and then fully weight bearing if pain free. Ankle exercises to regain range of motion were encouraged from 10 days postoperative; pool exercises and proprioceptive exercises were commenced from 3 weeks and impact activities from 5 weeks postoperative.

Clinical Research Findings
The presence or absence of tenderness on palpation over the ATFL, AiTFL, and deltoid ligament showed a highly significant relation between clinical and MRI findings of ligament injury (P < .0001). The presence of a combined injury to the AiTFL and deltoid ligament was highly predictive of a grade IIb injury; conversely, injury to the ATFL meant that the syndesmosis was less likely to be unstable
A positive squeeze test was associated with an increase in severity of injury, with the odds ratio of requiring surgery being 9.5 times greater if the squeeze test was positive. Not sure about how to conduct the squeeze test? Check it out here: https://www.youtube.com/watch?v=ThiW_9m7cFM
Return to sport
Grade IIa injuries -the mean time to return to sports was 45 days (range, 23 to 63 days), compared with 65 days (range, 27 to 104 days) for those with grade IIb injuries (P < .0001).
Patients with injury to both the AiTFL and deltoid ligament took longer to return to sports than those with an AiTFL injury alone, and IOL injury on MRI and PiTFL injury on MRI were both independently associated with a delay in return to sports. Conversely injury to the ATFL was associated with an earlier return to sports
Delay in return to sports was also associated with a positive squeeze test (64 days v 43 days, P < .0001) and a positive external rotation test (61 days v 43 days, P = .001). Although both tests had comparable sensitivity in predicting instability (79% and 76%, respectively), the specificity of the squeeze test was 71%, with a positive predictive value of 79% and negative predictive value of 68%, whereas for the external rotation test, the specificity was only 29%, with a positive predictive value of 61% and a negative predictive value of 50%.
Summary Findings
- Tenderness over individual ligaments during clinical examination 5 to 10 days after the initial injury correlated well with MRI confirmation of injury to these ligaments, and possibly more importantly, lack of tenderness was associated with normal MRI findings.
- Patients deemed to have a stable injury (isolated AiTFL rupture, even with a positive external rotation test) were treated conservatively, and all returned to sports at a mean time of 45 days
- Most patients with AiTFL and deltoid ligament tenderness together with positive squeeze and external rotation tests were found to have an unstable syndesmosis at arthroscopy.
- This study showed that a positive external rotation test is frequently found in a grade IIa injury, whereas the most predictive combination suggestive of instability is a positive squeeze test and concomitant injury to the medial deltoid ligament.
Keep in the loop
With the recent change in direction at the APA, it looks likely that AAP Education will be unable to advertise through InMotion or other APA publications any more. For this reason we will be primarily posting up to date course changes, short pieces and links of clinical importance onto our FaceBook page. Please take a second to LIKE this page via this LINK and in this way stay up to date.
✕
Subscribe for your FREE Mindsets email Course

Learn 4 Key Mindsets to be Successful in Private Practice
**Understanding Clients**
**Generate Referrals**
**Time Efficiency**
**3rd Party Payers**
You will receive, direct to your inbox 5 emails over 2 weeks