Trigger Finger Needling and Management
Abstract
A 2016 paper titled 'Acupuncture for the treatment of trigger finger in adults: a prospective case series' by Motohiro Inoue et al., reinforces what we treat in our Advanced Upper Quadrant Course in relation to managing digital stenosising tenosynovitis, or as it is commonly called 'trigger finger'. You can read the full abstract here: http://aim.bmj.com/content/early/2016/07/11/acupmed-2016-011068.abstract
Background
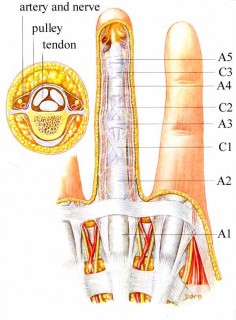
Trigger finger is a degenerative condition in which there is thickening of the restraining A1 pulley (A = annular ligamentous structure) and local inflammation (pain and swelling of synovial structures) resulting in catching of the long finger flexor tendon. This results in a painful snapping sensation on active extension of the associated finger or thumb. Common current management includes injections and surgical intervention.
Research Findings
This prospective study looked at 19 affected fingers (15 clients) and provided local daily treatment up to 5 times. In regards to the symptoms of pain and snapping they found;
- Significant improvements in both pain (measured using VAS) during snapping and severity of snapping directly after the first treatment (p<0.001)
- The pain level during snapping (measured before each treatment) improved over time, reaching statistical significance from the second treatment onwards (p<0.001)
- A significant improvement in the severity of snapping was observed from the second treatment (p<0.001).
In summary, there was an immediate improvement in pain and severity of snapping. It was proposed that pain relief was through activation of the diffuse noxious inhibitory control system and local opioid release systems, but the reduction in snapping would not be due to this mechanism. It is know that needling causes a local vasodilatory effect and in the case of recent (see below) trigger fingers, this may have reduced local tissue swelling, making the tendon less likely to catch.
Also of clinical interest was the effectiveness of treatment when measured in regards to duration of symptoms. Those that had greater than or equal to a 50% reduction in baseline symptoms (pain and snapping) had had their symptoms on average, 3 months or less. Those that had less than or equal to a 50% reduction in symptoms, had had their symptoms for 7 months on average.
Other Considerations
Management of this condition could be augmented by other tendon strategies;
- 1.During the treatment process, brace the finger, so that repeated catching of the tendon at the A1 pulley is prevented, reducing tendon aggravation (notable first thing in the morning)
- 2.Promote tendon remodeling, by implementing a several times a day, program of eccentric tendon loading, in a limited outer range to avoid irritation and snapping
- 3.Assist pain by implementing a program of isometric tendon exercises. Considerations: avoid tendon compression (choose appropriate angle), 45 second holds with 2-minute rest breaks and moderate to high load. Tweak these guidelines clinically. See http://www.bodyinmind.org/isometrics-tendon-pain/
✕
Subscribe for your FREE 10 Gems of Clinical Wisdom

Receive 10 emails of Clinical Wisdom
**High Ankle Injuries**
**Chronic Neck Pain**
**Fascial Manipulation**
**Ex. Prescription**
10 emails in 10 weeks. Receive your weekly inspiration of green clinical tea!