|

Infraspinatus is one of the more common muscles needled around the shoulder blade and a good one to start on because of the relative safety of solid bone as a depth stop. But wait you say, about 8% of the normal population have defective fossa floors (see 3D CTS picture). Clinically I would also add that a defect is probably more common in those over 60 years of age, due to osteoporosis and a general deconditioning in the upper limb with resultant bone loss in the scapular floor. Remember those undergraduate boxes of bones and how many had translucent scapular fossa floors? The concern in this situation is the potential of a pneumothorax or haemopneumothorax.
Yes we have to be careful, but as a result of this premise some instructors advise needling infraspinatus obliquely. I disagree with this approach. I agree that care needs to be taken, but needling obliquely seems not the optimal answer.
Lets look at the anatomy firstly.
To needle infraspinatus you may go through part of the posterior deltoid (#33 usually inserts in the middle 1/3 of the spine of the scapular). This would mean depth of around 5 - 10 mm depending upon muscle build over the middle of the scapular (most common trigger point zone). Depending upon your needling style, you may stay at the fascial boundary (greatest Aδ nociceptors concentration) or intramuscular (greatest type III nociceptors concentration). In all, direct depth to/into infraspinatus is 5 - 15 mm, with greater depths as you move laterally due to curvature of scapular, but less likelihood of a scapular defect.
To reach the lung/pleura field (#13) you would need to pass through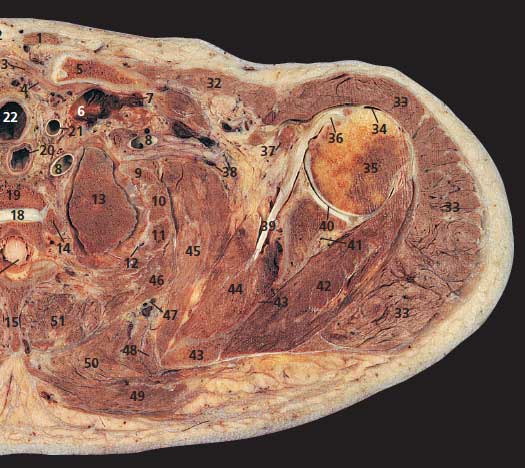 these two tissue (#33 & #42), the scapular floor (#43), subscapularis (#44), serratus anterior digitations (#45), plus navigate 2 ribs and adjoining intercostal muscles (#11 & #12). Looking at anatomical cross sections this would require penetration of around 40 - 65mm, again depending upon body build, which always needs to be taken into account. I would suggest that if you have placed a needle 40mm into ‘infraspinatus’ on a thinish person and thinking this an appropriate depth, then you are at the wrong course. This is one reason why AAP Education conducts wet lab anatomy workshops; so professionals can update their anatomy skills. Like any other core skill anatomy requires refreshing on a regular basis. these two tissue (#33 & #42), the scapular floor (#43), subscapularis (#44), serratus anterior digitations (#45), plus navigate 2 ribs and adjoining intercostal muscles (#11 & #12). Looking at anatomical cross sections this would require penetration of around 40 - 65mm, again depending upon body build, which always needs to be taken into account. I would suggest that if you have placed a needle 40mm into ‘infraspinatus’ on a thinish person and thinking this an appropriate depth, then you are at the wrong course. This is one reason why AAP Education conducts wet lab anatomy workshops; so professionals can update their anatomy skills. Like any other core skill anatomy requires refreshing on a regular basis.
Now Consider Practicality & Geometry
To minimise this possibility instructors have advised oblique needling. However this causes additional issues. Firstly when you insert a needle at an angle, it is more difficult to penetrate the protective skin layer. Think upper atmosphere and light penetration. More light penetrates at the equator (warmer) and greater amounts reflected as you move towards the poles.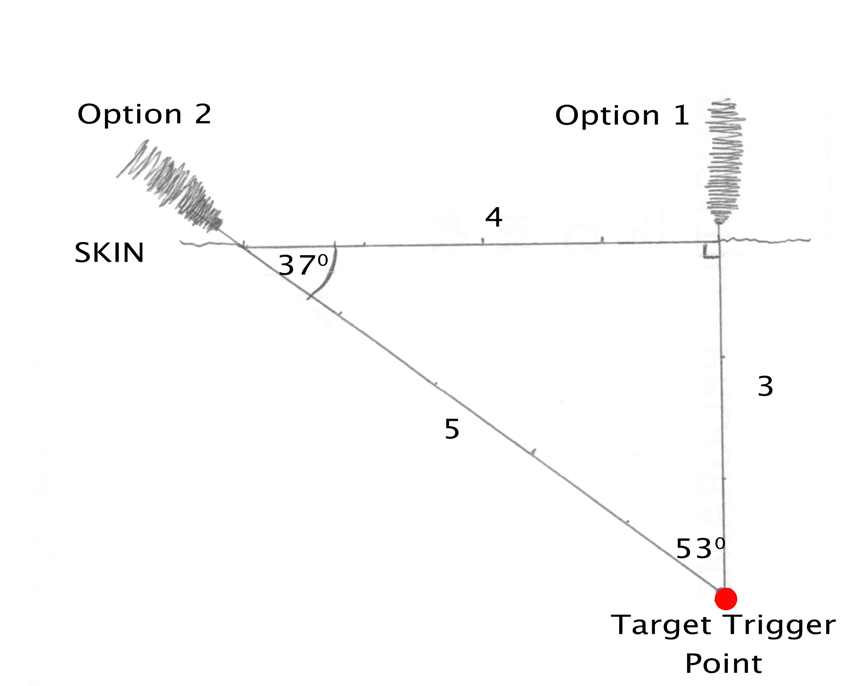
The other issue to consider is that as you increase the angle of insertion away from the perpendicular (Option 1), the length of needle to penetrate to desired point increases (Option 2). Think a 3-4-5 triangle or ‘right triangle’ from school. If the trigger point is 3 units in perpendicular depth from the skin and you move your needle insertion to gain an oblique angle of insertion for ‘safety’. At an angle of 37 degrees (4 units from Option 1) it will now take a 50mm needle to reach your trigger point. With increased depth comes increased inaccuracy. Just what you don’t want when targeting a tissue 1-2mm in size.
The simplest approach is often the direct approach, with the proviso of the relevant anatomy and taking into consideration your client’s body shape. This is a example of the clinical reasoning applied for all techniques taught on our dry needling and acupuncture courses.
Cross sectional picture used is reproduced from Human Sectional Anatomy 2nd Edition by Ellis, Logan and Dixon, with kind permission of Hodder Education.
All the best,
Doug Cary FACP
Specialist Musculoskeletal Physiotherapist (awarded by Australian College of Physiotherapy, 2009)
PhD Candidate Curtin University
Clinical Director AAP Education
email: [email protected]
ph/fx: 08 90715055
Receive a FREE Information Report

Choose The Top 5 Manual Therapy Apps or Infection Control & Needling (V2)
Along with the report you'll also get a complimentary subscription to "Clinical Kit" our regular eZine (email newsletter) and Free Bronze Membership. You'll get ideas, information, insight and inspiration on a regular basis, plus access to our Resource Library, helping you unravel those clinical conundrums appearing every day.
You are free to use material from the Blog in whole or in part, as long as you include complete attribution, including live website link. Please also notify me where the material will appear. The attribution should read: "By Doug Cary FACP of AAP Education. Please visit our website at www.aapeducation.com.au for additional clinical articles and resources on post graduate education for health professionals" (Please make sure the link is live if placed in an eZine or in a web site.)
HOME | DRY NEEDLING PROGRAM | CERVICAL SPINE | FASCIAL MANIPULATION | MULLIGANS | MSK & RT ULTRASOUND | NEURODYNAMIC SOLUTIONS | THE SHOULDER | VESTIBULAR PROGRAM | LIVING ANATOMY WET LABS | BLOG
   
|
