Have you treated a Quadratus Femoris? Here is my first experience

Case Summary:
A 51-year-old male commercial painter presented with a 2-day history of right-sided lumbar and lateral buttock pain radiating to the lateral thigh. He couldn't identify a clear onset but had been painting a house (involving ladders, squatting, and awkward positions) and moving furniture the day before. He went to bed without issues but woke with mild soreness, which worsened throughout the day. No paresthesia or numbness was reported.
Pain Characteristics:
- Aggravated by: Sitting, sit-to-stand, sidelying (either side)
- Relieved by: Supine position, walking
- Medication: Tried Voltaren with no effect
Objective Findings:
- Pain Level: 5/10 (Numeric Rating Pain Scale)
- Lumbar Movements: Full range, no neural provocation tests +ve
- Hip Movements: Pain-limited flexion; increased pain with adduction (20° vs. normal 40°) and external rotation (30° vs. normal 50°). Internal rotation and quadrant tests were normal.
- Isometric Tests: No pain in any direction at 90° hip flexion
- Palpation: Tenderness over L4-L5 and L2-L3, and posterior/distal to the greater trochanter (~5 cm) (see green crosses on image). Gluteals and piriformis were non-tender.
Unusual Finding:
Painful restriction in hip adduction and external rotation—atypical for this type of presentation.
Diagnosis & Intervention:
Given the negative lumbar and neural findings and localized tenderness, a quadratus femoris strain was suspected.
Treatment:
- Dry needling with a 0.25 x 40 mm Seirin needle in the tender area (contralateral sidelying, hip flexed and adducted). A strong local twitch was elicited at 35 mm depth.
- Advised to avoid single-leg activities and taught hip stretches.
Outcome:
At the 2-day follow-up, the patient was pain-free and comfortable with all activities of daily living (ADLs). Rehabilitation progressed with single-leg squats, bridges, and balance drills over the next 6-8 weeks.
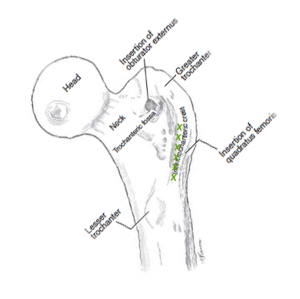
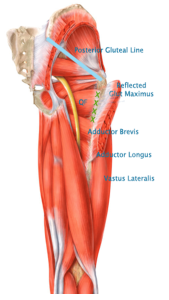
Anatomy Review:
The quadratus femoris is a rectangular muscle connecting the ischium (medially) to the quadrate tubercle of the femur (laterally), along the intertrochanteric crest. It lies beneath the inferior gemellus and posterior to the obturator externus. It is innervated by the nerve to quadratus femoris (L4-S1). The myotendinous junction is the most common site of injury.
Background:
Quadratus femoris strain is an uncommon musculoskeletal condition, often diagnosed via MRI (unavailable locally in Esperance). Research suggests a higher female-to-male ratio, non-traumatic onset, and diagnosis delays from 1 day to 5 months. Clinically, pain can manifest in the groin, lateral thigh, or posterior thigh and is aggravated by squatting or sitting. NSAIDs generally provide little relief.
Typical findings include pain with passive flexion, adduction, internal rotation, and weakness in external rotation. However, external rotation weakness was absent in this case, making the presentation unique.
Conclusion:
This case provided new insights into quadratus femoris strain presentations. The unusual restriction of adduction and external rotation will inform my future assessments.
Further Reading:
- O'Brien & Bui-Mansfield: MRI of Quadratus Femoris Muscle Tear: Another Cause of Hip Pain
- Bano et al.: Persistent sciatica induced by quadratus femoris muscle tear and treated by surgical decompression: A case report.Journal of Medical Case Reports, 2010, 4:236
Comment for this post has been locked by admin.