The Invisible Injury: Treating Ultrastructural Muscle Tears with Dry Needling
Given we love our football so much, it seems appropriate to combine this with my fascination with 'Magic Muscles'. Hamstring injury is where these two loves intersect, so I have dived a bit deeper into the underlying structural deficit and why they can 'heal' so fast. Included at the end is a protocol that combines the dry needling approach with rehab, as we all know that combined therapists provide the best outcomes. Love to hear your thoughts on the blog here.
1. IntroductionMuscle strain injuries represent a major challenge in sports medicine, causing widespread training disruptions across elite and recreational sports. Traditionally, these injuries are seen as macro-structural failures, in which muscle fibres are visibly torn, resulting in bruising. Such damage is easily identified using magnetic resonance imaging (MRI) or high-resolution ultrasound (US). However, clinicians frequently encounter a confusing scenario: an athlete presents with acute, localised muscle pain, weakness, and tenderness, yet shows a completely normal or "negative" structural scan on MRI. This mismatch points directly to ultrastructural muscle injuries. These are microscopic lesions occurring at the deep cellular level that escape standard cross-sectional macro-imaging. Despite the lack of structural disruption, these injuries impair performance and require targeted care. Among treatments, dry needling has gained strong clinical support. This blog explores ultrastructural injuries, evaluates the unique diagnostic landscape, and reviews how dry needling facilitates rapid functional recovery.
2. The Pathophysiology of Ultrastructural Muscle TearsTo understand an ultrastructural tear, one must look past the gross anatomy of the muscle belly and focus on the microscopic architecture of the sarcomere—the basic contractile unit of skeletal muscle. Skeletal muscle consists of bundles of muscle fibres housing myofibrils. These myofibrils contain the contractile proteins actin and myosin, organised sequentially between boundaries known as Z-discs. Ultrastructural injuries involve microscopic damage isolated to the sarcolemma (the muscle cell membrane), the Z-discs, and the delicate cytoskeletal anchors that stabilise the contractile matrix. These micro-tears are typically driven by intense eccentric exercise, where a muscle lengthens while under active tension. During high-velocity eccentric actions, the mechanical load applied to the individual myofibrils can exceed the tensile capacity of the proteins. This results in the physical pulling apart or "streaming" of the Z-discs and localised disruptions in the sarcolemma.
Crucially, in a true ultrastructural injury, the basal lamina (the cell's basement membrane backing) remains fully intactBecause the global framework of the muscle tissue is preserved, there is no macroscopic hematoma, fascial tear, or prominent fluid retraction to alter tissue density on an MRI. However, the micro-disruption of the sarcolemma triggers a cellular emergency. Intracellular contents leak, and extracellular calcium rushes into the cell, inducing localised inflammation, edema, and a protective muscular spasm.
3. The Diagnostic Paradox: Elite Athlete Imaging and RatiosThe clinical reality of these invisible micro-tears is strongly supported by sports medicine literature examining elite, high-velocity athletes. The Australian Football League (AFL) represents an ideal case study, given that Australian Rules football demands repeated, maximum-velocity sprinting, rapid acceleration, and high-kicking actions—mechanisms that subject the hamstring complex to extreme eccentric stress. Multi-year tracking data from the Soft Tissue Injury Registry of the AFL (STRAFL) shows that hamstring strains remain the single highest injury burden in the sport, averaging roughly 7 injuries per club each season. Foundational studies first revealed that approximately 31% to 45% of elite football players presenting with clear clinical criteria for an acute hamstring tear showed completely negative MRIs.
[Modern 3.0-T MRI / High-Res US Framework]
├──► ~70-75%: Positive Macro-Structural Landmarks (Mjunction fluid, fiber tears)
└──► ~25-30%: Negative Macro-Structural Scan (True Ultrastructural Micro-Tears)
Modern sports medicine continues to validate this "negative scan" phenomenon. Even with the widespread adoption of high-field 3.0-Tesla (3.0-T) MRI machines, which offer vastly superior structural resolution over older 1.5-T scanners, up to 25% to 30% of acute, highly symptomatic hamstring strains continue to show no structural tear or fluid disruption. Furthermore, when clinicians use real-time diagnostic ultrasound, the negative predictive value drops, missing 15% to 27% of injuries that present with profound clinical symptoms. In contemporary classification systems (such as the British Athletics Muscle Injury Classification), these are categorised as Grade 0 injuries: clinical muscle strains with completely normal imaging. Crucially, AFL data indicates that these imaging-negative, ultrastructural injuries achieve a significantly faster return-to-play timeline—averaging roughly 6.6 days compared to over 20 days for macroscopic, MRI-positive tears. This rapid recovery is possible because the intact basal lamina allows for streamlined cellular repair without the need to clear large hematomas or lay down extensive scar tissue.
4. Dry Needling as a Targeted Therapeutic InterventionBecause the muscle's macroscopic framework remains structurally stable during an ultrastructural injury, the primary therapeutic goal shifts.
Rather than protecting a large mechanical gap, clinicians must focus on alleviating secondary neuromuscular guarding by optimising the direct insertion of solid filament needles into hypertonic skeletal muscle tissue or myofascial trigger points.When a muscle sustains ultrastructural damage, surrounding intact fibres undergo an involuntary contraction. This localised guarding is a protective mechanism mediated by the central nervous system to limit movement. However, prolonged guarding compromises capillary blood flow, resulting in localised hypoxia and persistent ischemic pain.
[Ultrastructural Tear] ► [Neuromuscular Guarding] ► [Ischemia/Hypoxia] ► [Delayed Repair]
▲ (Dry Needling Interrupts Here)
The physiological impact of dry needling on an ultrastructural injury operates through three primary pillars:
- Neuromuscular Reset: Inserting a needle into a guarding muscular band elicits a local twitch response (LTR). This involuntary spinal reflex immediately disrupts the dysfunctional, hyperactive loop of acetylcholine release at the motor endplate, lifting the protective spasm and restoring optimal resting length.
- Biochemical and Microvascular Restoration: Dry needling instantly alters the chemical environment of the injured tissue. It reduces the local concentration of nociceptive substances and pro-inflammatory cytokines while triggering a localised release of nitric oxide. This sudden vasodilation flushes out trapped metabolic byproducts and delivers fresh, oxygenated blood directly to the struggling sarcomeres.
- Accelerated Remodelling: By piercing the localised region, the needle triggers a controlled, microscopic inflammatory response. This stimulus upregulates the recruitment of satellite cells (skeletal muscle stem cells), which migrate to the disrupted sarcomeres and accelerate the synthesis of new actin and myosin proteins.
When deploying dry needling for an ultrastructural tear, timing is critical. In the acute phase (1–3 days post-injury), direct needling into the exact epicentre of the micro-tear should be avoided to prevent mechanical irritation to the delicate, leaking sarcolemma. Instead, practitioners should target the peripheral guarding zones—the hypertonic bands of the muscle complex that are compensating for the injury. As the injury transitions into the sub-acute phase (day 4 onwards), gentle needling can be safely introduced closer to the affected zone to maximise microvascular recruitment.In conclusion, ultrastructural muscle injuries represent a subtle yet highly disruptive category of sports trauma. As highlighted by professional AFL data, a lack of visible pathology on a modern 3.0-T MRI does not equate to a lack of genuine clinical impairment. Instead, these invisible injuries consist of microscopic disruption of the sarcomeres, paired with profound neuromuscular guarding.
Dry needling serves as an elegant, targeted intervention for these injuries. By interrupting protective neural spasms, restoring local capillary perfusion, and promoting satellite cell recruitment, dry needling addresses the precise physiological demands of the micro-torn muscle, helping athletes safely and efficiently bridge the gap from cellular trauma back to peak performance.
📑 References- Whalan, M., Lovell, R., & Sampson, J. A. (2024). Epidemiology of hamstring strain injuries in elite male Australian football players: An analysis of 773 injuries over 7 seasons from the STRAFL registry. JOSPT Open, 2(4), 289–296. https://www.jospt.org/doi/10.2519/josptopen.2024.0359
- Verrall, G. M., Slavotinek, J. P., Barnes, P. G., Fon, G. T., & Spriggins, A. J. (2001). Clinical risk factors for hamstring muscle strain injury: a prospective study with correlation of injury by magnetic resonance imaging. British journal of sports medicine, 35(6), 435–440. https://doi.org/10.1136/bjsm.35.6.435
- Warren, P., Gabbe, B. J., Schneider-Kolsky, M., & Bennell, K. L. (2010). Clinical predictors of time to return to competition and of recurrence following hamstring strain in elite Australian footballers. British Journal of Sports Medicine, 44(6), 415–419. https://doi.org/10.1136/bjsm.2008.048181
- Zein, M. I., Reurink, G., Suskens, J. J. M., Monte, J. R. C., Smithuis, F. F., Buckens, S., Maas, M., & Tol, J. L. (2025). 3.0-Tesla MRI Observation at Return to Play After Hamstring Injuries. Clinical Journal of Sport Medicine: official journal of the Canadian Academy of Sport Medicine, 35(2), 119–126. https://doi.org/10.1097/JSM.0000000000001289
- Hirahata, Y., Yasui, Y., Sasahara, J., Inui, T., Nakagawa, T., Kawano, H., & Miyamoto, W. (2025). Role of Ultrasonography and MRI in Acute Hamstring Strains: Diagnostic and Prognostic Insights. Diagnostics15(9), 1053. https://doi.org/10.3390/diagnostics15091053
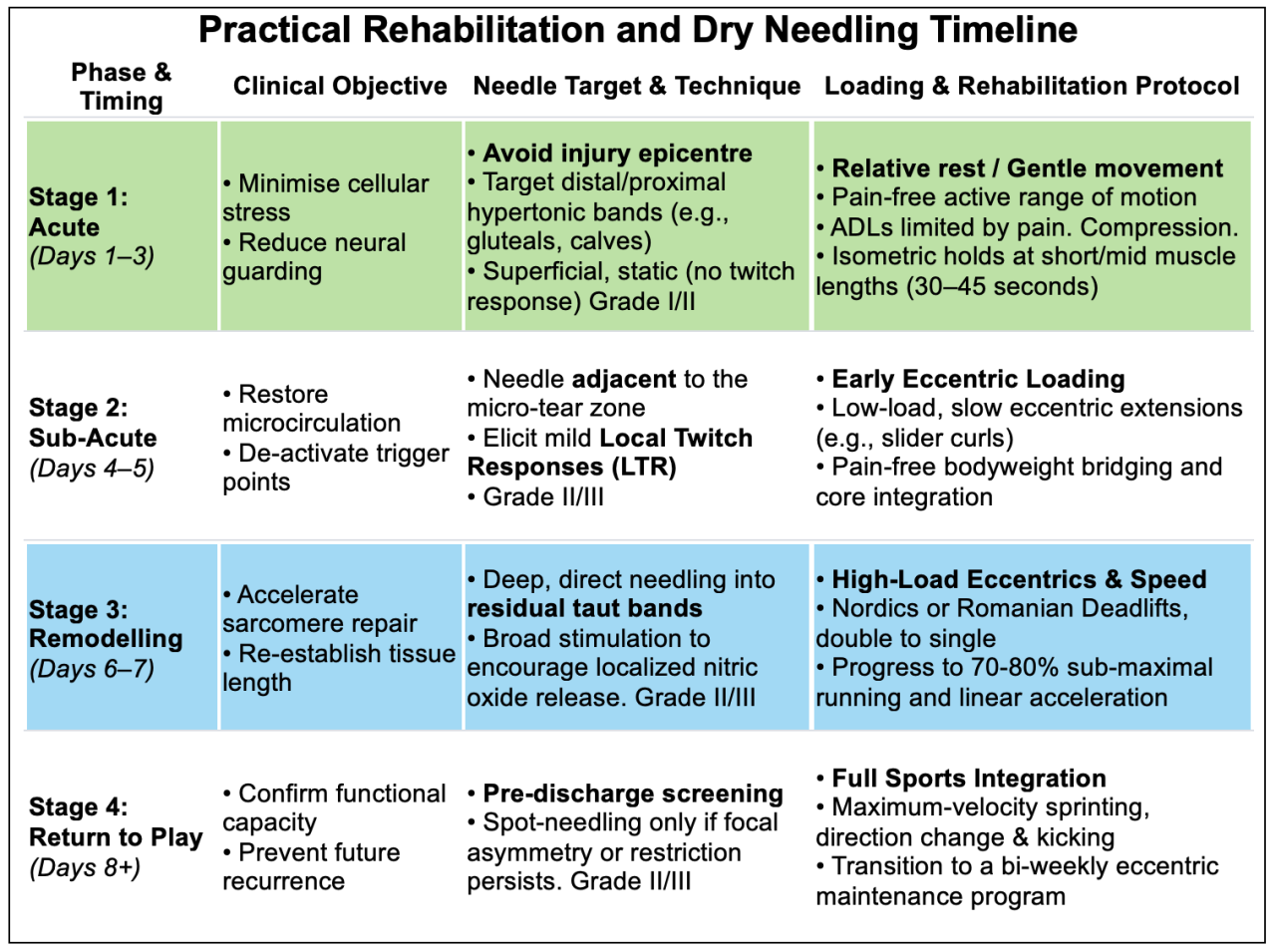
Dry needling and rehabilitation guideline
Do you follow a similar treatment plan for those magic muscles that you encounter?
Comment for this post has been locked by admin.